Mountain View, Missouri (West Plains / Willow Springs / Winona / Cabool / Summersville) ---- Spinal Decompression Doctor, Russell Schierling, presents another blog article on Spinal Decompression Therapy.
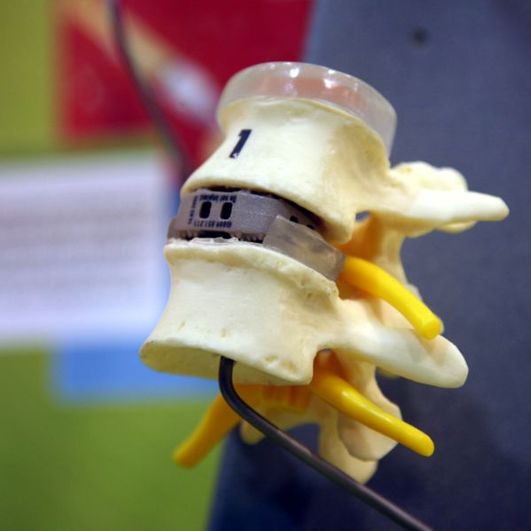
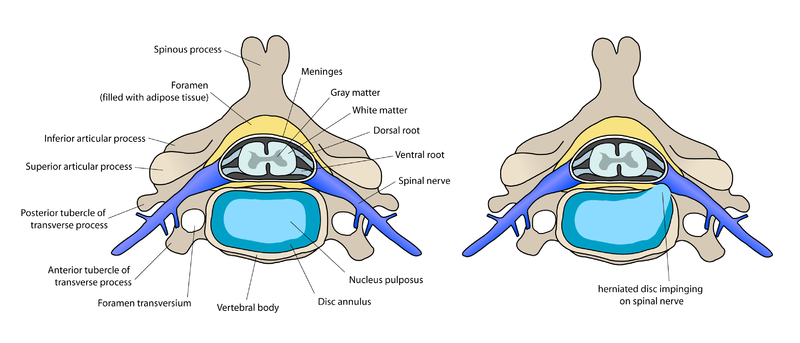
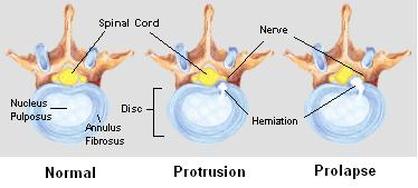
HERNIATED DISC
or
PIRIFORMIS SYNDROME?
or
PIRIFORMIS SYNDROME?
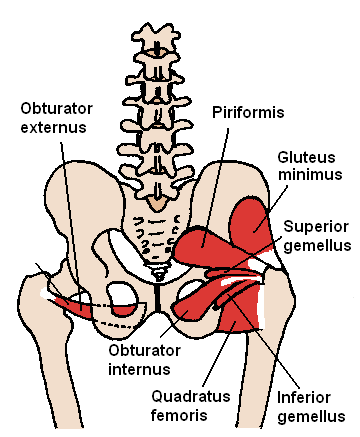
Image by Beth Ohara
|
OR
|

Image by User:Tonbi_ko
|
Answering this question is critical because these are two very different problems that must be treated completely differently from each other --- yet can produce nearly identical symptoms.
But is this question being answered correctly the majority of the time? I'll answer this with a quote from a recent research project from UCLA's Cedars Sinai Medical Center in collaboration with the Institute for Nerve Medicine. The study was published in in a 2005 edition of the Journal of Neurosurgery: Spine. "Most spine specialist consider Piriformis Syndrome to be extremely rare. However, the authors conclude that although it is rarely diagnosed, it is actually a common cause of sciatica - possibly as common as the well known herniated disk syndromes." "Rarely Diagnosed". This is still true in my neck of the woods. When you look at the VIDEO TESTIMONIALS of people I have treated with 20 - 40 year histories of Piriformis Syndrome, an almost universal thread is that none of them had ever as much as heard of PS until they came into my office. Not that it would have mattered. I am not convinced that doctors making the correct diagnosis is helping these people in any meaningful way. If you have suffered with PIRIFORMIS SYNDROME, you know what I am talking about.
But is this question being answered correctly the majority of the time? I'll answer this with a quote from a recent research project from UCLA's Cedars Sinai Medical Center in collaboration with the Institute for Nerve Medicine. The study was published in in a 2005 edition of the Journal of Neurosurgery: Spine. "Most spine specialist consider Piriformis Syndrome to be extremely rare. However, the authors conclude that although it is rarely diagnosed, it is actually a common cause of sciatica - possibly as common as the well known herniated disk syndromes." "Rarely Diagnosed". This is still true in my neck of the woods. When you look at the VIDEO TESTIMONIALS of people I have treated with 20 - 40 year histories of Piriformis Syndrome, an almost universal thread is that none of them had ever as much as heard of PS until they came into my office. Not that it would have mattered. I am not convinced that doctors making the correct diagnosis is helping these people in any meaningful way. If you have suffered with PIRIFORMIS SYNDROME, you know what I am talking about.
IKE REESE'S THIRTY YEAR'S OF MISERY ENDS IN ONE TEN MINUTE TREATMENT!
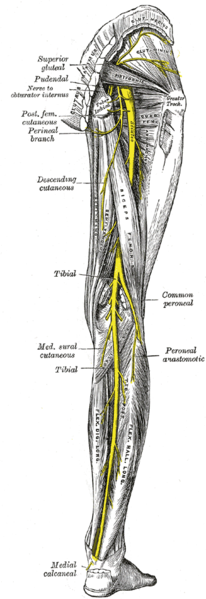
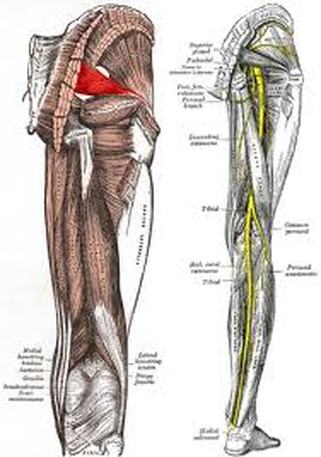
THE PIRIFORMIS MUSCLE & SCIATIC NERVE
|
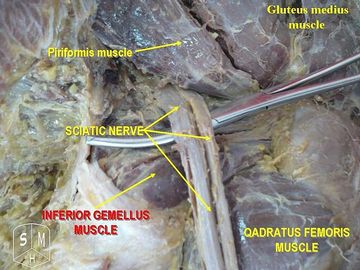
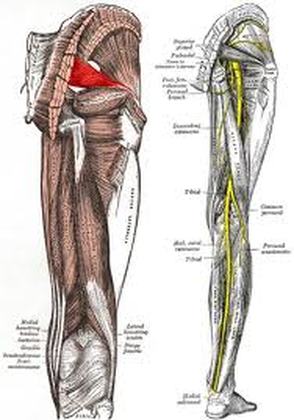
Photo by Anatomist90
LEFT: Gray's Anatomy, Right Leg. Note the Piriformis Muscle (red) found just above the beginning of the large (yellow) sciatic nerve. Piriformis Syndrome frequently involves a deep aching in the buttock, as well as sciatica (pain, numbness, tingling, into the leg). ABOVE: Note the Sciatic Nerve underneath the Piriformis Muscle.
|
The Piriformis Muscle (piriformis means “pear shaped“) is a tiny muscle located deep in the buttocks, underneath the gluteal (butt) muscles. This little muscle is the most well-known of a group of muscles known as the “Hip Rotator Cuff” and is frequently the source of pain in the butt and associated Sciatica. I have had several people come to me for Spinal Decompression Therapy that actually had Piriformis Syndrome. Yes, we saved them a lot of time, grief, and money. Spinal Decompression Therapy does not help Piriformis Syndrome!
Piriformis Syndrome is a miserable condition in which the Piriformis Muscle becomes overly tight. Although there are almost always underlying biomechanical issues to deal with (bow legged or knock knees, high / low arches, a history of PULLED MUSCLES around the pelvis, etc) this pathological tightness of the Piriformis is usually the result of FASCIAL ADHESIONS or TENDINOSIS.
Piriformis Syndrome can be aggravated by bending, lifting, sitting, sports, and even driving (foot on the gas pedal). Contrary to what your M.D. might tell you, there are no drugs or surgery that are effective for treating Piriformis Syndrome. I will warn you, in 20 plus years of practice I have never one time seen a person whose Piriformis Release Surgery actually worked.
Piriformis Syndrome is an extremely common condition, and is far more likely to be found in women than men (about 12-15 times more often). Although I can only speculate on the reason for this, I suspect that it is a child-bearing issue. It probably also has to do with the naturally wider shape of a woman’s pelvis. This is the most likely explanation for my finding it much more frequently in women than men — even in women who have not had children.
PIRIFORMIS SYNDROME CAUSES SCIATICA
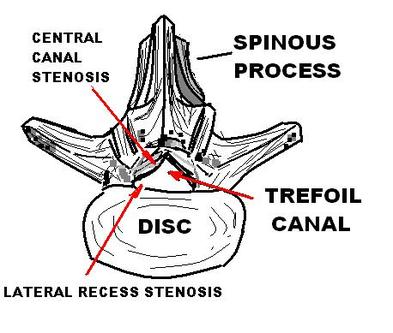
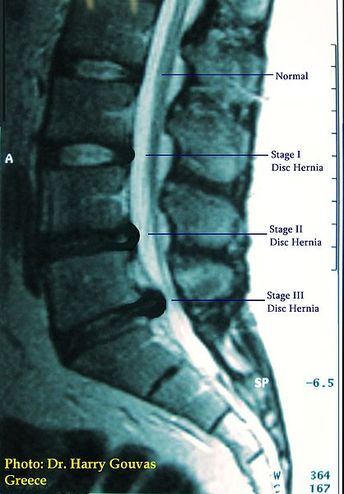
As I stated earlier, Piriformis Syndrome is a major cause of sciatica (leg pain, numbness, tingling, or weakness, in any combination), hip pain, and buttock pain. Because sciatica is so often involved, the problem is often misdiagnosed as a HERNIATED DISC, DEGENERATIVE DISC, or sacroilliac problem (sometimes chronic sacroilliac problems are related to problems in the Piriformis Muscle).
The SCIATIC NERVE is both the largest and longest nerve in the body, and at its largest point is about the thickness of one’s thumb. The sciatic nerve originates in the low back (lumbar spine region) and angles toward the middle of the buttock. It then extends down through the leg, passing just underneath the piriformis muscle. Be aware that in as much as half the population, the sciatic nerve travels through the Piriformis Muscle, passes over the Piriformis Muscle, or splits in two and passes directly around the Piriformis Muscle.
Be aware that much of what is called Piriformis Syndrome is actually a Piriformis Tendinopathy. See our TENDINOSIS PAGE for more information. Usually this pain will be worse at the hip joint itself (lower, outer buttock region).
The symptoms of Piriformis Syndrome usually begin as a deep aching in what women like to refer to as their “hip” area. This pain will be found along an imaginary line that runs from the very tip top of the butt crack, to the greater trochanter of the hip bone (the bony knob on the upper and portion of the outer or lateral thigh).
People most predisposed to chronic contracture and microscopic scarring of the piriformis muscle, are people who wear cruddy or improper footwear for their foot type (high-arched people wearing a “stability” or “dual-density” shoe), those with faulty spinal or lower limb mechanics, overweight or obese people, those with poor posture, people who spend too much time sitting, too much time on concrete, or not getting enough physical activity (or occasionally too much exercise — overtraining). And of course, the biggie — just being female.
Due to mechanical stresses causing chronic tightness / contracture, the Piriformis Muscle can actually become shortened over time. This often results in microscopic scarring of the fascial sheaths that tightly surround the muscle itself. Piriformis Syndrome is most commonly worse at rest (sitting or lying down) and is often (but not always) temporarily relieved by moderate activity (particularly walking or stretching).
Visit our MICROSCOPIC SCAR TISSUE & FASCIAL ADHESIONS page to understand the relationship of Fascial Membranes to Muscles.
For years, I did not really understand why I had such good clinical results with so many cases of buttock / hip pain and sciatica, while other seemingly identical cases were largely unresponsive to chiropractic adjustments. Frequently these “problem” cases would get fantastic short-term results from their adjustment, but these results never seemed to last more than a few days at the most (and often no more than a few hours). It was not until I started doing “TISSUE REMODELING” in 2001, that I truly began to understand what was going on.
Over the past decade I have come to realize that Piriformis Syndrome is literally “epidemic” in the female portion of our society (see our PATIENT TREATMENT DIARY); with the medical community being largely mystified about what it really is, or how to treat it effectively. Again, drugs and surgery do not constitute “effective treatment” for Piriformis Syndrome. Never assume that a “Piriformis Release Surgery” will solve your problems, as many people who have it are worse.
As you have read on our Fascial Adhesions Page, scar tissue is normal, elastic tissue (think nicely combed hair here) that has been disrupted from its organized structure, into a balled-up and tangled wad of inflexible and hyper-sensitive, micro-gristle (think of a hair tangle that cannot be combed out). This kind of microscopic scar tissue is not typically seen in the muscle itself, but in the fascia. Fascia is the thin, but very tough, yellowish white membranes that cover muscles. In my neck of the Ozarks, deer hunters call these membranes, “Striffin“.
Fascia is arguably the single most pain-sensitive tissue in the body! Fascial Adhesions will cause pain and dysfunction. Destroy Fascial Adhesions and Destroy Chronic Pain!
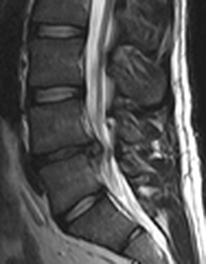
Because most of these scar tissues are in the fascia as opposed to the muscle itself, they do not image on MRI --- period. It is my opinion that microscopic scarring of the Piriformis Muscle is the single most common cause of chronic, long-standing, Sacroilliac or buttock pain (the Sacroilliac Joints are the bony bumps that lie just up and lateral to the top of the butt crack). It is also the most common cause of what I have for years referred to in the office as a “butt-based” sciatica.
PIRIFORMIS SYNDROME & YOUR FEET
If you have extra-high arches or “fallen” arches, or if you have abnormal lower body biomechanics of any sort; you probably need arch supports (orthotics). We carry some nice, generic orthotics that will work for many people. However, some of you will require custom orthotics. Allow me to give you an example of why:
Although I have seen my fair share of Piriformis Syndrome patients with fallen arches or flat feet, as far as I can tell from clinical experience, high arches seem to be more related to Piriformis Syndrome. The higher the arch, the more you get “pushed” onto the outside of your foot. To see what this does to the Piriformis Muscle; stand up, put your hands on your upper buttocks in the area of the Piriformis Muscle. Now, roll your weight out onto the outsides of your feet. Notice how the Piriformis Muscle instantly becomes tight as a drum? This is what is going on all day long if you have improperly supported high arches. And there is only one company on the planet that I am aware of that specifically specializes in shoe inserts (orthotics) for people with high arches……. XF
The only custom orthotic company that I recommend for my patients is X-treme Footworks out of Idaho Springs, CO. To find out whether your pain is Disc related, or Piriformis Syndrome, simply call us at (417) 934 6337 to schedule a free consultation with Doctor Schierling. It is imprtant to differentiate Piriformis Syndrome from Disc problems because Piriformis Syndrome will not respond well to Spinal Decompression Therapy --- in fact, it will usually make it worse.
_
Piriformis Syndrome is a miserable condition in which the Piriformis Muscle becomes overly tight. Although there are almost always underlying biomechanical issues to deal with (bow legged or knock knees, high / low arches, a history of PULLED MUSCLES around the pelvis, etc) this pathological tightness of the Piriformis is usually the result of FASCIAL ADHESIONS or TENDINOSIS.
Piriformis Syndrome can be aggravated by bending, lifting, sitting, sports, and even driving (foot on the gas pedal). Contrary to what your M.D. might tell you, there are no drugs or surgery that are effective for treating Piriformis Syndrome. I will warn you, in 20 plus years of practice I have never one time seen a person whose Piriformis Release Surgery actually worked.
Piriformis Syndrome is an extremely common condition, and is far more likely to be found in women than men (about 12-15 times more often). Although I can only speculate on the reason for this, I suspect that it is a child-bearing issue. It probably also has to do with the naturally wider shape of a woman’s pelvis. This is the most likely explanation for my finding it much more frequently in women than men — even in women who have not had children.
PIRIFORMIS SYNDROME CAUSES SCIATICA
As I stated earlier, Piriformis Syndrome is a major cause of sciatica (leg pain, numbness, tingling, or weakness, in any combination), hip pain, and buttock pain. Because sciatica is so often involved, the problem is often misdiagnosed as a HERNIATED DISC, DEGENERATIVE DISC, or sacroilliac problem (sometimes chronic sacroilliac problems are related to problems in the Piriformis Muscle).
The SCIATIC NERVE is both the largest and longest nerve in the body, and at its largest point is about the thickness of one’s thumb. The sciatic nerve originates in the low back (lumbar spine region) and angles toward the middle of the buttock. It then extends down through the leg, passing just underneath the piriformis muscle. Be aware that in as much as half the population, the sciatic nerve travels through the Piriformis Muscle, passes over the Piriformis Muscle, or splits in two and passes directly around the Piriformis Muscle.
Be aware that much of what is called Piriformis Syndrome is actually a Piriformis Tendinopathy. See our TENDINOSIS PAGE for more information. Usually this pain will be worse at the hip joint itself (lower, outer buttock region).
The symptoms of Piriformis Syndrome usually begin as a deep aching in what women like to refer to as their “hip” area. This pain will be found along an imaginary line that runs from the very tip top of the butt crack, to the greater trochanter of the hip bone (the bony knob on the upper and portion of the outer or lateral thigh).
People most predisposed to chronic contracture and microscopic scarring of the piriformis muscle, are people who wear cruddy or improper footwear for their foot type (high-arched people wearing a “stability” or “dual-density” shoe), those with faulty spinal or lower limb mechanics, overweight or obese people, those with poor posture, people who spend too much time sitting, too much time on concrete, or not getting enough physical activity (or occasionally too much exercise — overtraining). And of course, the biggie — just being female.
Due to mechanical stresses causing chronic tightness / contracture, the Piriformis Muscle can actually become shortened over time. This often results in microscopic scarring of the fascial sheaths that tightly surround the muscle itself. Piriformis Syndrome is most commonly worse at rest (sitting or lying down) and is often (but not always) temporarily relieved by moderate activity (particularly walking or stretching).
Visit our MICROSCOPIC SCAR TISSUE & FASCIAL ADHESIONS page to understand the relationship of Fascial Membranes to Muscles.
For years, I did not really understand why I had such good clinical results with so many cases of buttock / hip pain and sciatica, while other seemingly identical cases were largely unresponsive to chiropractic adjustments. Frequently these “problem” cases would get fantastic short-term results from their adjustment, but these results never seemed to last more than a few days at the most (and often no more than a few hours). It was not until I started doing “TISSUE REMODELING” in 2001, that I truly began to understand what was going on.
Over the past decade I have come to realize that Piriformis Syndrome is literally “epidemic” in the female portion of our society (see our PATIENT TREATMENT DIARY); with the medical community being largely mystified about what it really is, or how to treat it effectively. Again, drugs and surgery do not constitute “effective treatment” for Piriformis Syndrome. Never assume that a “Piriformis Release Surgery” will solve your problems, as many people who have it are worse.
As you have read on our Fascial Adhesions Page, scar tissue is normal, elastic tissue (think nicely combed hair here) that has been disrupted from its organized structure, into a balled-up and tangled wad of inflexible and hyper-sensitive, micro-gristle (think of a hair tangle that cannot be combed out). This kind of microscopic scar tissue is not typically seen in the muscle itself, but in the fascia. Fascia is the thin, but very tough, yellowish white membranes that cover muscles. In my neck of the Ozarks, deer hunters call these membranes, “Striffin“.
Fascia is arguably the single most pain-sensitive tissue in the body! Fascial Adhesions will cause pain and dysfunction. Destroy Fascial Adhesions and Destroy Chronic Pain!
Because most of these scar tissues are in the fascia as opposed to the muscle itself, they do not image on MRI --- period. It is my opinion that microscopic scarring of the Piriformis Muscle is the single most common cause of chronic, long-standing, Sacroilliac or buttock pain (the Sacroilliac Joints are the bony bumps that lie just up and lateral to the top of the butt crack). It is also the most common cause of what I have for years referred to in the office as a “butt-based” sciatica.
PIRIFORMIS SYNDROME & YOUR FEET
If you have extra-high arches or “fallen” arches, or if you have abnormal lower body biomechanics of any sort; you probably need arch supports (orthotics). We carry some nice, generic orthotics that will work for many people. However, some of you will require custom orthotics. Allow me to give you an example of why:
Although I have seen my fair share of Piriformis Syndrome patients with fallen arches or flat feet, as far as I can tell from clinical experience, high arches seem to be more related to Piriformis Syndrome. The higher the arch, the more you get “pushed” onto the outside of your foot. To see what this does to the Piriformis Muscle; stand up, put your hands on your upper buttocks in the area of the Piriformis Muscle. Now, roll your weight out onto the outsides of your feet. Notice how the Piriformis Muscle instantly becomes tight as a drum? This is what is going on all day long if you have improperly supported high arches. And there is only one company on the planet that I am aware of that specifically specializes in shoe inserts (orthotics) for people with high arches……. XF
The only custom orthotic company that I recommend for my patients is X-treme Footworks out of Idaho Springs, CO. To find out whether your pain is Disc related, or Piriformis Syndrome, simply call us at (417) 934 6337 to schedule a free consultation with Doctor Schierling. It is imprtant to differentiate Piriformis Syndrome from Disc problems because Piriformis Syndrome will not respond well to Spinal Decompression Therapy --- in fact, it will usually make it worse.
_










 RSS Feed
RSS Feed
