Mountain View, Missouri (West Plains / Willow Springs / Winona / Cabool / Summersville) ---- Spinal Decompression Doctor, Russell Schierling, presents another blog article on Spinal Decompression Therapy.
HERNIATED DISCS
A Picture (and several videos) Is Worth a Thousand Words
A Picture (and several videos) Is Worth a Thousand Words
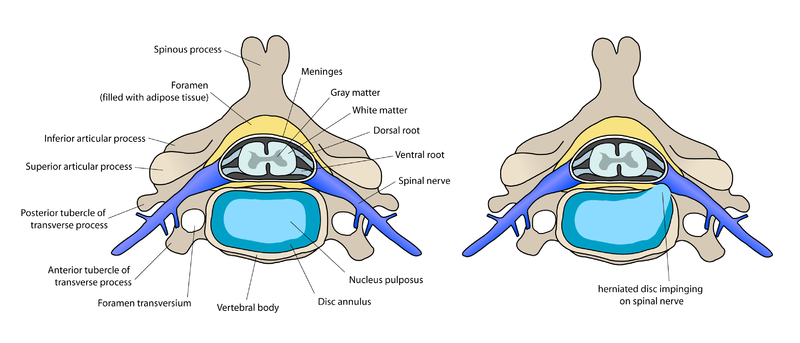
Image by user:debivort
In the spine, there are 24 vertebrates. In between these vertebrates are cushions called Intervertebral Discs. If you'll notice the two pictures above, the picture of the one on the right is different from the one on the left. On the right picture, the round aqua blue portion (the disc) is bulging back and pressing on the spinal nerve (blue). This is a Herniated Disc. But before we delve into the in's, out's, how's, and why's of Herniated Discs and what it takes to fix them, let's first touch on what a normal disc is, what it looks like, and how it behaves.
Spinal Discs have several functions, but two stand out above the others.
Spinal Discs have several functions, but two stand out above the others.
- They create space inside the Intervertebral Foramen:
- They act as a "cushion" or "bushing" between the vertebrates:
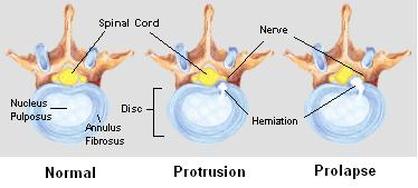
- The Outer Annulus: The outer layer (or more appropriately, "layers") of the disc is called the Annulus Fibrosus and is made up of lots and lots of ligaments. If you were to look at a Spinal Disc under a microscope, you would notice that the Annular Ligaments wrap around and around and around the center of the disc. This is because The Annulus job is to hold The Nucleus (the jelly center) in place. How does it do this? Think of a baseball here. If you have ever cut open a baseball (or even an old golf ball), you will find lots and lots of rubber bands coiled around a center core. Only instead of a core made of rubber or cork, the disc's core is made up of jelly.
- The Inner Nucleus: The Nucleus, technically called the Nucleus Pulposus, is the jelly-like center of the disc. Because it is a thick jelly-like fluid, it has the ability to push outwards in all directions. Bend to one side, and the disc tends to push toward the other. Bend forward, and the nuclear jelly pushes toward the back of the disc.
Anything that encroaches on the Intervertebral Foramen (IVF) will compete with the nerve for space. As you can imagine, it is not a good thing for the nerve to be pressed or encroached upon. It's pretty easy to understand that the nerve needs a certain amount of room as it comes through the bony window we call the IVF. When the nerve does not have the room it needs to stretch and move, it can become "pinched" or severely irritated. As you can also imagine, this is not a good thing either. How does this happen? Follow along as I walk you through the process.
As the Spinal Discs bear loads, the pressure pushes the nucleus outward in all directions. If there is a weak spot in the disc's outer Annulus, its most inner layers (near the Nucleus) begin to tear. As they tear, the jelly center (The Nucleus) begins to push its way toward the outside. Bear in mind that Disc Herniations rarely happen in the front part of the disc. Because people tend to lean forward (not backward) and bend side to side, the pressure tends to push the nucleus toward the back of the disc. This is where discs tend to rupture --- to the back and just lateral of the midline ---- where the spinal cord and spinal nerves are.
Full-blown Disc Herniations rarely happen all at once. Much more common is a Progressive Disc Injury (diagram below). As the disc is continually stressed, the annulus continues to tear just a little bit more; allowing the nucleus "slip" a little bit more ---- always creating a little bit bigger bulge and putting a just little bit more pressure on the nerve. But then it heals some, and might even feel better for awhile. In other words, it's not an "all-or-none" proposition. It is usually a process where a disc goes from normal to ruptured over time ---- even though the terrible pain might have come on all at once.
And while you will hear terms bantered around such as "Slipped Disc," "Herniated Disc," Ruptured Disc," "Prolapsed Disc", etc, the question to ask is whether the disc is Contained or Non-Contained. As long as the Nucleus is at least mostly contained within the Annulus, there is a strong possibility that conservative measures such as Spinal Decompression Therapy can help you avoid surgery. But if the Nucleus slips completely outside of the Annulus ---- a "Non-Contained" lesion...... Unfortunately, you might have a surgical problem on your hands. Unless your neurosurgeon says otherwise (AND MAYBE EVEN AGAINST THEIR WISHES), as long as you do not have severe leg weakness and / or loss of bladder or bowel function, you might want to consider Spinal Decompression Therapy!
As the Spinal Discs bear loads, the pressure pushes the nucleus outward in all directions. If there is a weak spot in the disc's outer Annulus, its most inner layers (near the Nucleus) begin to tear. As they tear, the jelly center (The Nucleus) begins to push its way toward the outside. Bear in mind that Disc Herniations rarely happen in the front part of the disc. Because people tend to lean forward (not backward) and bend side to side, the pressure tends to push the nucleus toward the back of the disc. This is where discs tend to rupture --- to the back and just lateral of the midline ---- where the spinal cord and spinal nerves are.
Full-blown Disc Herniations rarely happen all at once. Much more common is a Progressive Disc Injury (diagram below). As the disc is continually stressed, the annulus continues to tear just a little bit more; allowing the nucleus "slip" a little bit more ---- always creating a little bit bigger bulge and putting a just little bit more pressure on the nerve. But then it heals some, and might even feel better for awhile. In other words, it's not an "all-or-none" proposition. It is usually a process where a disc goes from normal to ruptured over time ---- even though the terrible pain might have come on all at once.
And while you will hear terms bantered around such as "Slipped Disc," "Herniated Disc," Ruptured Disc," "Prolapsed Disc", etc, the question to ask is whether the disc is Contained or Non-Contained. As long as the Nucleus is at least mostly contained within the Annulus, there is a strong possibility that conservative measures such as Spinal Decompression Therapy can help you avoid surgery. But if the Nucleus slips completely outside of the Annulus ---- a "Non-Contained" lesion...... Unfortunately, you might have a surgical problem on your hands. Unless your neurosurgeon says otherwise (AND MAYBE EVEN AGAINST THEIR WISHES), as long as you do not have severe leg weakness and / or loss of bladder or bowel function, you might want to consider Spinal Decompression Therapy!
 |  user:debivort |
CARDINAL SIGNS OF A HERNIATED DISC
Of course you can and probably should go for an MRI. However, we know that 50% of the general population has disc herniations that show up on MRI's, but cause no pain or overt symptoms (HERE). I am interested in physical findings that indicate a disc injury. There are three Cardinal Signs that I look for in determining if someone might have at least some degree of Disc Herniation. They are.....
- ANTALGIA: An antalgic posture is leaning to one side or the other (or to the front). If the Nucleus Pulposus "slips" or herniates to the right, most of the time people will lean to the left, and vise versa. This is an automatic reaction of the body as it tries to pull you off of, or away from the bulging nucleus. Often times you will notice that the belly button is pulled away from the body's center line.
- POSITIVE VALSALVA or DeJARINE SIGN: This is pain that occurs specifically when you cough, sneeze, or strain on the stool. When you cough, sneeze, or strain, you develop a great deal of momentary internal pressure. Because force always takes the path of least resistance, the pressure released by a cough or sneeze pushes on the injured (bulging) portion of the disc. I frequently hear people tell me that if they know they are going to cough or sneeze, they hold themselves up on a counter or table so their legs do not collapse out from under them in sheer pain. Speaking of legs......
- SCIATICA: The nerves from either side of your low back area grow together into one nerve ---- the Sciatic Nerve. The Sciatic Nerve is not only the longest nerve in the body, it is the biggest as well (as big as your finger). If you cause pressure on one of the nerves that makes up the Sciatic Nerve, you can end up in a world of hurt. This can be in the form of pain. But it can also be in the form of numbness, tingling, weakness, odd sensations (paresthesia), etc. Sometimes the pain will do odd things like start at the knee and go down, or skip certain areas. SCIATICA can manifest itself in an almost endless variety of ways. It can mimic knee or hip problems as well.

ANTALGIA POSITIVE VALSALVA or DeJARINE SIGN SCIATICA
(leaning away from pain) (severe pain when coughing or sneezing) (leg symptoms)
(leaning away from pain) (severe pain when coughing or sneezing) (leg symptoms)
PIRIFORMIS SYNDROME:
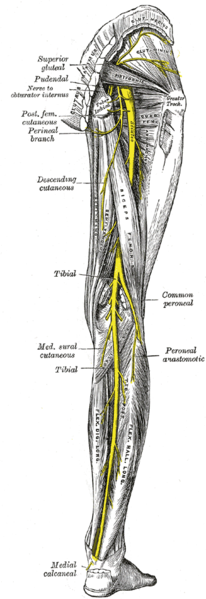
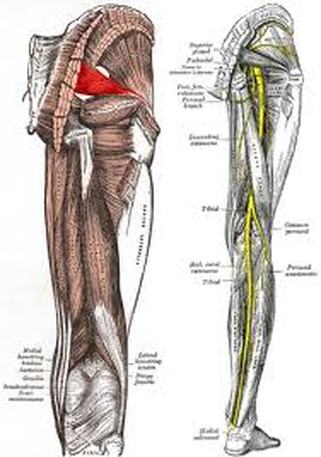
One quick word about Piriformis Syndrome. Piriformis Syndrome is literally a "pain in the butt" that can sometimes mimic a disc problem ---- even though it is caused by a problem with a muscle. If you have little or no low back pain but lots and lots of buttock pain (or chronic Sacroilliac pain), this might very well be your problem ---- especially if you are female (notice the relationship of the Piriformis Muscle and the Sciatic Nerve in the picture below). To understand the difference between a Herniated Disc and Piriformis Syndrome, please take three minutes and visit www.DestroyPiriformisSyndrome.com.
One quick word about Piriformis Syndrome. Piriformis Syndrome is literally a "pain in the butt" that can sometimes mimic a disc problem ---- even though it is caused by a problem with a muscle. If you have little or no low back pain but lots and lots of buttock pain (or chronic Sacroilliac pain), this might very well be your problem ---- especially if you are female (notice the relationship of the Piriformis Muscle and the Sciatic Nerve in the picture below). To understand the difference between a Herniated Disc and Piriformis Syndrome, please take three minutes and visit www.DestroyPiriformisSyndrome.com.
MRI'S
OF
HERNIATED DISCS
This MRI is a lateral view of a person facing to your left. The ling white line is the spinal cord. The white areas on the left of the MRI are discs. The fact that they are white indicates that they have water in them ---- a good thing. Notice the circled area of one of the discs rupturing into the spinal cord. The one below it is rupturing as well. The disc is not white. It is gray, fading to black. This is indicative of a disc that is dehydrated.
 Image by User:Tonbi_ko | 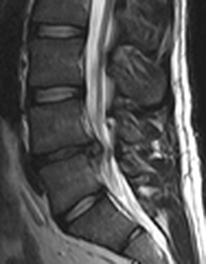 Image by Edave |
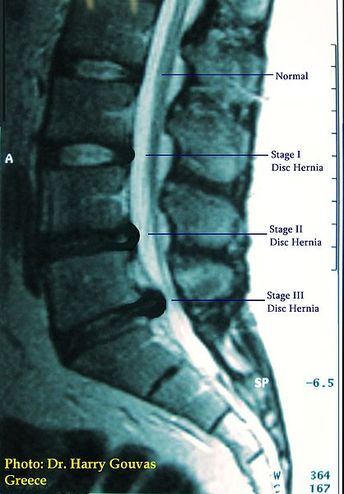
You can see the same thing in this MRI of the L4 Disc. Notice how it is not only bulged, but is thinning as well. This is called SPINAL DEGENERATION. Note that the healthy discs are white on MRI, but the herniated discs are much darker, depending on their degree of degeneration. This is a really good MRI to study. It shows the progression of disc problems. It starts with a normal disc at the L1-L2 disc, and ends with a Stage III Disc Herniation at L5-S1.
DO NOT HAVE SURGERY WITHOUT TRYING CONSERVATIVE METHODS FIRST!
Have you been diagnosed with a Herniated Disc? Maybe you have the Three Cardinal Signs of a Herniated Disc. Whatever the case, DO NOT under any circumstances consent to spinal surgery without a second opinion. Check out the internet message boards on the subject. Visit the online support groups for people suffering from Failed Spinal Surgery Syndrome (FSSS). Or better yet, talk to people you know who have had spinal surgery. Ask them how they have done. I promise you that over half of those you interview would not do it again ---- even if you paid them!
Call us today (417) 934-6337 to set up a free consultation with Dr. Schierling to see if Spinal Decompression Therapy MIGHT BE RIGHT FOR YOU and your specific problem.
Call us today (417) 934-6337 to set up a free consultation with Dr. Schierling to see if Spinal Decompression Therapy MIGHT BE RIGHT FOR YOU and your specific problem.



 RSS Feed
RSS Feed
