 | Mountain View, Missouri (West Plains / Cabool / Winona / Summersville / Willow Springs) ---- Spinal Decompression Doctor, Russell Schierling, presents another blog article on Spinal Decompression Therapy. |
“My Doctor Says that since I don’t have Leg Pain, I do not have a Disc Problem.”
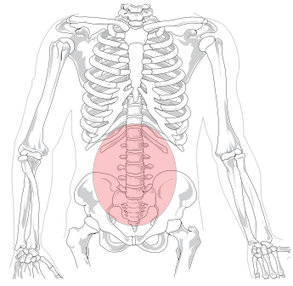
Wow, have I heard this one a lot of times! This is a common misconception by doctors, PT's, and even chiropractors, who do not extensively deal with severe Spinal Disc problems such as DISC HERNIATIONS, SPINAL STENOSIS, or DEGENERATIVE DISCS on a day to day basis. Much of this goes back to what doctors learned in school. If you have leg pain (SCIATICA), you have a disc problem ---- if you do not have leg lain, your disc is not the problem. The same thing can be said of the relationship of the Spinal Disc to low back pain. I actually see a fair number of people who have severe buttock / leg pain, yet have no low back pain whatsoever. Is it from the Disc, or is it something else?
Just like individual fingerprints, the reality is that no two bodies are exactly the same. Professors present lectures, and text books present anatomical pictures of the way that various structures in the body should look. We know how different people look from one another on the outside. The truth is that because everyone is so different on the inside, nerves are not always found exactly where one would expect them to be. In fact, when it comes to studying human anatomy, anomalies and anatomical variations are the norm. Discs can herniate in any number of common (or very uncommon) patterns. When you throw in the phenomenon of ASYMPTOMATIC DISC HERNIATIONS, the conundrum gets even bigger. You may be starting to understand why back surgeries can be such a crap shoot.
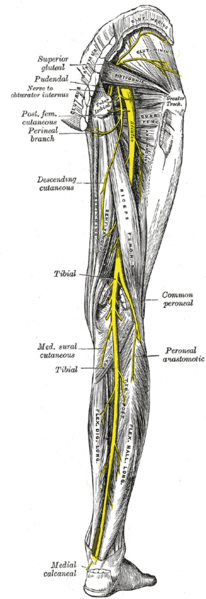
Another potential monkey wrench in the machine is that Sciatica is frequently (about 40% of the time) caused by non-disc problems like PIRIFORMIS SYNDROME. Like I insinuated earlier, Sciatica has the ability to manifest itself in an almost endless array of patterns.
- It can affect various parts of the leg
- It can skip parts of the leg, while affecting other parts.
- Sometimes it will cause problems below the knee, but not above the knee.
- Sometimes sciatica will not travel below the knee.
- Sometimes it might just stay in the buttock region.
- Sometimes a person might have terrible leg symptoms ---- and absolutely ZERO low back pain (fairly common).
- Sometimes people have lots of low back pain but no Sciatica-like symptoms in their leg (also fairly common). These people may or may not have a disc problem that can be verified on MRI (see the previous link on Asymptomatic Herniations).
A great deal of research tells us that much low back pain can actually come from the disc itself (as opposed to the HERNIATED NUCLEUS PULPOSUS) pressing on a nerve. This is why so many of the MRI's that show one or more Disc Bulges, Ruptures, or Herniations, cannot always be trusted. What do I mean buy this? Doctors have known for years that OVER HALF THE ADULT POPULATION IS WALKING AROUND WITH DISC BULGES ---- that are not causing any symptoms at all! This is because many doctors have forgotten that the outer fibers of the disc (THE ANNULUS FIBROSIS) actually have their own nerve supply (and potential pain source). Usually this type of pain is on or very near the spine's mid-line. Patients will typically describe this pain as a deep, nagging ache that can be sharp and severe if you move just right.
All of this is important to know. Why should you know this information? Because it can often times be difficult to trust your doctor to be looking out for your best interests. What do I mean by this? Try explaining the fact that every study on back surgery is freakier than the study that came out before it. There is a steady stream of research telling us that SPINAL SURGERIES HAVE POOR OUTCOMES. This is verified by viewing internet message boards, or talking to patients who have had back surgery. Why is it that SPINAL FUSIONS ----- the worst of the worst offenders ----- have increased nearly 1,600% since 2003; even though results are typically terrible? Why not ask your specialist who is recommending the surgery?
Fortunately there is new technology available that has the potential to PUT A SOLID GOLD BRICK in your hands ----- without surgery or those nasty CORTICOSTEROID INJECTIONS that dramatically speed up the degenerative processes working on your spine. It's called Non-Surgical Spinal Decompression Therapy, and it could be just the thing for you. Because I see lots of desperate people looking for any glimmer of hope for their conditions, I run into a fair number of people who are not good candidates for Spinal Decompression Therapy. Although many of these are people I am simply UNABLE TO HELP, many I can help ---- without having to go through our SPINAL DECOMPRESSION PROGRAM ----- HERE is an example.
To find out whether or not Spinal Decompression Therapy MIGHT BE A GOOD OPTION for your particular problem, simply call our office at (417) 934-6337 to set up a free consultation with Dr. Schierling. He will look at your tests, discuss your history, and give you his honest opinion. If he can help you he will. If he cannot, he will try to provide you with the best options.












 RSS Feed
RSS Feed